Hair ConstitutionConstitution Facts
Hair ConstitutionConstitution Facts DownloadsRequirements, Instructions
DownloadsRequirements, Instructions VideosWatch Amazing Videos
VideosWatch Amazing Videos Why Choose Dr. Keser?Top Reasons to Choose Dr.KeserDr. Keser in MediaDr. Keser On TV Shows
Why Choose Dr. Keser?Top Reasons to Choose Dr.KeserDr. Keser in MediaDr. Keser On TV Shows Medicines for hair loss can slow thinning of hair and increase coverage of the scalp by growing new hair and enlarging existing hairs. But they need to be taken regularly. If you stop the medicine, hair loss returns. Do not expect to regrow a full head of hair. Hair coverage is improved on the top of the head, but not on the forehead area.
Medicines for hair loss can slow thinning of hair and increase coverage of the scalp by growing new hair and enlarging existing hairs. But they need to be taken regularly. If you stop the medicine, hair loss returns. Do not expect to regrow a full head of hair. Hair coverage is improved on the top of the head, but not on the forehead area.
Hair Loss: Should I Take Medicine to Regrow Hair?
Medication choices
Medicines often used to treat inherited hair loss include:
 Symptoms of Hairloss
Symptoms of HairlossDifferent types of hair loss have different symptoms. Sometimes, both the head and body can be affected.
Male-pattern baldness usually starts around the late twenties or early thirties. By their late thirties, most men have some degree of hair loss.
Male-pattern baldness is so called because it generally follows a set pattern. The first stage is usually a receding hairline, followed by thinning of the hair on the crown and temples. This can leave a horseshoe shape of hair around the back and sides of the head. Sometimes it can progress to complete baldness, although this is uncommon.
Women's hair gradually thins with age, but women generally lose hair from the top of their head only. This is usually more noticeable after the menopause (when a woman's periods stop at around 52 years of age).
Alopecia areata causes patches of baldness about the size of a large coin. They usually appear on the scalp but can occur anywhere on the body.
There are usually no other symptoms, although in around one in 10 people the fingernails may also be affected, and may have a pitted or grooved appearance.
In most cases of alopecia areata, hair will grow back in a few months. At first, hair may grow back fine and white, but over time it should thicken and regain its normal colour.
Some people with alopecia areata go on to develop a more severe form of hair loss, such as:
As scarring alopecia is caused by another health condition, you will have symptoms relating to this condition besides hair loss. Unlike other forms of hair loss, the skin where the hair has fallen out is likely to be affected in some way.
For example, in cases where lichen planus has caused scarring alopecia, the skin may develop an itchy rash and may be inflamed.
In scarring alopecia, the hair follicles (small holes in the skin that contain the roots of each hair) are damaged and replaced with scar tissue. This means that new hair cannot grow, so the hair loss is permanent.
Anagen effluvium, most commonly caused bychemotherapy, usually occurs quickly. In most cases, hair loss is noticeable within a few weeks of chemotherapy starting. In anagen effluvium, hair loss is widespread, rather than in patches. As well as losing hair from your scalp, you may also lose hair from your body and face.
This type of hair loss is usually temporary. Your hair should stop falling out and start to grow back a few months after chemotherapy has stopped.
In telogen effluvium, there is widespread hair loss from your scalp, rather than specific bald patches. Your hair may feel thinner than before, but you are unlikely to lose it all. Your other body hair will not usually be affected.
In most cases of telogen effluvium, your hair will stop falling out and start to grow back within six months.
The Norwood classification, published in 1975 by Dr. O’tar Norwood, is the most widely used classification for hair loss in men. It defines two major patterns and several less common types (see the chart below). In the regular Norwood pattern, two areas of hair loss–a bitemporal recession and thinning crown–gradually enlarge and coalesce until the entire front, top and crown (vertex) of the scalp are bald.
 |
Class I represents an adolescent or juvenile hairline and is not actually balding. The adolescent hairline generally rests on the upper brow crease. |
 |
Class II indicates a progression to the adult or mature hairline that sits a finger’s breath (1.5cm) above the upper brow crease, with some temporal recession. This also does not represent balding. |
 |
Class III is the earliest stage of male hair loss. It is characterized by a deepening temporal recession. |
 |
Class III Vertex represents early hair loss in the crown (vertex). |
 |
Class IV is characterized by further frontal hair loss and enlargement of vertex, but there is still a solid band of hair across the top (mid-scalp) separating front and vertex. |
 |
Class V the bald areas in the front and crown continue to enlarge and the bridge of hair separating the two areas begins to break down. |
 |
Class VI occurs when the connecting bridge of hair disappears leaving a single large bald area on the front and top of the scalp. The hair on the sides of the scalp remains relatively high. |
 |
Class VII patients have extensive hair loss with only a wreath of hair remaining in the back and sides of the scalp. |
(Left) Typical Norwood Class V showing two distinct areas of hair loss with the bridge of hair separating the front and back thinning significantly. (Right) Class VI showing the confluence of the front a back to form one bald area.
The Norwood Class A patterns are characterized by a front to back progression of hair loss. Norwood Class A’s lack the connecting bridge across the top of the scalp and generally have more limited hair loss in the crown, even when advanced.
The Norwood Class A patterns are less common than the regular pattern (< 10%), but are significant because of the fact that, since the hair loss is most dramatic in the front, the patients look very bald even when the hair loss is minimal. Men with Class A hair loss often seek surgical hair restoration early, as the frontal bald area is not generally responsive to medication and the dense donor area contrasts and accentuates the baldness on top. Fortunately, Class A patients are excellent candidates for hair transplantation.
(Left) Norwood Class IVa with anticipated hairline drawn. (Right) Early Class Va with some residual hair on the top of the scalp. Note that in both stages there is a complete absence of hair in the front part of the scalp. In both Norwood patterns, the sides and back tend to resist androgenetic changes, although the sides may exhibit significant thinning in old age (senile alopecia.)
Two other types of genetic hair loss in men not often considered by doctors, “Diffuse Patterned Alopecia” and “Diffuse Unpatterned Alopecia,” pose a significant challenge both in diagnosis and in patient management. Understanding these conditions is crucial to the evaluation of hair loss in both men and women, particularly those that are young when the diagnoses may be easily missed, as they may indicate that a patient is not a candidate for surgery.
Diffuse Patterned Alopecia (DPA) is an androgenetic alopecia manifested as diffuse thinning in the front, top and crown, with a stable permanent zone. In DPA, the entire top of the scalp gradually miniaturizes (thins) without passing through the typical Norwood stages. Diffuse Unpatterned Alopecia (DUPA) is also androgenetic, but lacks a stable permanent zone and affects men much less often than DPA. DUPA tends to advance faster than DPA and end up in a horseshoe pattern resembling the Norwood class VII. However, unlike the Norwood VII, the DUPA horseshoe can look almost transparent due to the low density of the back and sides. Differentiating between DPA and DUPA is very important because DPA patients often make good transplant candidates, whereas DUPA patients almost never do, as they eventually have extensive hair loss without a stable zone for harvesting.
The progression of male hair loss in Diffuse Patterned Alopecia (DPA) and Diffuse Unpatterned Alopecia (DUPA). In DUPA, the sides thin significantly as well.
In order to elucidate the reasons and treatment modalities of hair loss, hair constitution, and hair quality should be defined.
Hair on human body has a role of sustaining body temperature, protecting the body against external factors, contributing sensation, and complementing aesthetic appearance of the body. Except in the palm, sole, and glans penis, hair can be found in all surfaces of human body in varying thickness and color.
Terminal hairs are the thickest. Hair, beard, and chest hair are of this kind.
Hair is produced and grows in a layer called 'hair follicle', which surrounds the hair and also called 'hair root'. Unlike common belief, hair does not constantly grow. The growth ceases at one point and then falls out. In the place of hair lost, a fresh hair is produced through hair follicle. This process, which is referred to as 'the life-cycle of hair', successively continues in 3 stages (click here for figure).
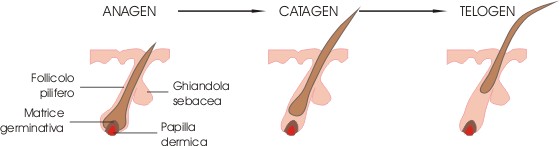
Head scalp contains approximately 100.000 hairs, 85-90 % of which are in anagen stage and 10-15% of which are in katagen and telogen stages. An average of 100-150 hair fall-outs a day is considered a normal physiological process. Contrary to common belief, frequent shaving does not increase the hair growth or density. In anagen stage, the mean hair growth is 0.37 mm. At the end of growth stage, hair may grow as much as 25-100 cm ( in men, down to the back; in women, down to waistline)
In hair loss, the duration of the stages mentioned is shorter.
We help you make your trip to Turkey as easy and hassle-free as possible. We offer free airport transfers from/to the airport with English speaking guide. We take care of arranging your accommodation for night of your hair transplantation. We will be happy to meet with you to discuss any questions you may have about a hair transplant in Turkey. Free Consultation...
For information about the latest and most modern fue hair transplant and hair loss treatment available, schedule your no-obligation consultation with Dr. Keser today. - Learn More about FUE...